Wolff-Parkinson White Syndrome (WPW) and Atrioventricular reciprocating tachycardia (AVRT)
Overview
“Wolff-Parkinson White syndrome (WPW)”, refers to a condition where an accessory, or extra, connection exists between the top atria and the bottom ventricles present in less than 1% of the general population, with an associated tachyarrhythmia, or fast heart rhythm. The diagnosis of a “WPW pattern or EKG” reflects those patients with an accessory, or extra, atrioventricular connection, but no diagnosis or symptoms of a fast heart rhythm.
At this point a short review of the normal conduction system, as described in the “Your Heart”section, is in order. The sinus node, a structure in the high right atrium, depolarizes typically 60 to 100 times per minute sending an electrical impulse throughout both atria to the AV node. In brief, this leads to synchronized biatrial contraction before ventricular contraction forces blood out of the heart into the circulation. The AV node, a structure that sits in the middle of the heart, is normally the only electrical connection between the atria and the ventricles. The AV node serves as a traffic signal, controlling the rate of electrical impulses from the atria allowed to reach the ventricle, limiting the danger of 1 to 1 conduction of fast rhythms from the atrium to the ventricles.
Humans can be born with extra electrical connections, or tissue, otherwise known as “accessory pathways” that lead to alternative mechanisms for conduction from the atria to the ventricles. These connections are typically severed during the normal human heart development in a fetus. In rare cases where these connections are not lost, they may persist into birth and ultimately adulthood. Still again, many of these connections, or accessory pathways, can be benign and disappear over time.
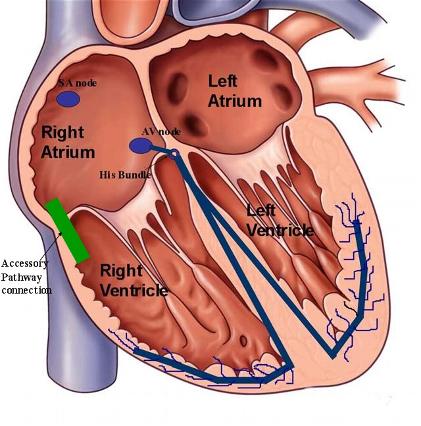
Figure 1. Image of the normal conduction system of the heart including the AV node and distal bundle branches. The green bar represents the presence of an accessory pathway that is able to conduct electrical signals directly from the atria, inserting into the ventricles, and independent of AV nodal conduction.
Because accessory pathways insert directly into the ventricular tissue from the atria, and are located outside and away from the AV node, they allow for direct 1 to 1 conduction from the atria to the ventricles with each sinus impulse. This is the sign of a “WPW pattern or EKG” on the surface 12-lead EKG performed by your physician. As seen below, there is typically a “slurred”, or broadened upslope (called a delta wave) present in the EKG leads that hints to the existence of an accessory pathway and represents its abnormal depolarization and preexcited electrical capture of the ventricles. The WPW EKG pattern represents a prexcitation of the ventricles, meaning there is premature electrical depolarization of the ventricles since this tissue does not typically have the properties of the AV node (i.e, like a traffic signal) in slowing 1 to 1 conduction from the top to bottom chambers. Your physician can use the directionality, shape, and other qualities of this delta wave to help localize the site of insertion of the accessory pathway connection to the bottomventricles. This can be important to dictate the strategy of elimination of these accessory pathways in those patients who choose to pursue or need a “curative” catheter ablation procedure (described below).
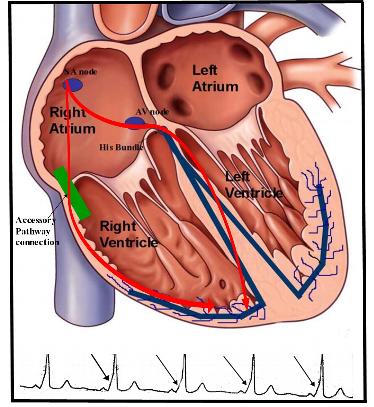 Figure 2. Image of preexcitation of the EKG with a manifest accessory pathway leading to the EKG findings of WPW pattern. As seen here, electrical conduction from the atria to the ventricles can occur via the normal AV nodal system and the accessory pathway simultaneously. This leads to the creation of the slurred upstroke, or delta wave, seen on the surface EKG lead and denoted by arrows in the tracing seen here.
Figure 2. Image of preexcitation of the EKG with a manifest accessory pathway leading to the EKG findings of WPW pattern. As seen here, electrical conduction from the atria to the ventricles can occur via the normal AV nodal system and the accessory pathway simultaneously. This leads to the creation of the slurred upstroke, or delta wave, seen on the surface EKG lead and denoted by arrows in the tracing seen here.
As you can imagine, the existence of an accessory pathway to the ventricles, can lead to the necessary conditions to create a tachycardia-circuit “loop” reentry rhythm, with the accessorypathway as one limb and the normal AV node as the second limb. Even other arrhythmias, such as atrial tachycardia, atrial fibrillation, and atrial flutter can use these accessory pathways preferentially at faster heart rates to electrically stimulate the ventricles in an abnormal, preexcited fashion. An SVT that uses this accessory pathway to conduct to the ventricles results in the clinical diagnosis of WPW, or prexcitation syndrome (as opposed to the isolated WPW EKG pattern).
The most second most common type of SVT, is called orthodromic atrioventricular reentrant tachycardia (AVRT). As eluded to above, in this form of SVT, the sinus electrical impulse propagates in the usual fashion from the atria to the AV node and to the ventricles (antegrade direction). However, now with the existence of an abnormal accessory pathway, this electrical impulse can propagate in the reverse direction (retrograde) from the ventricles to the atria,completing an electrical “reentry” circuit. This type of tachycardia, orthodromic AVRT, appears as a narrow-complex SVT on the 12-lead EKG (often similar to an EKG of AVNRT leading to its difficulty in diagnosis with patient symptoms similar to other SVT).
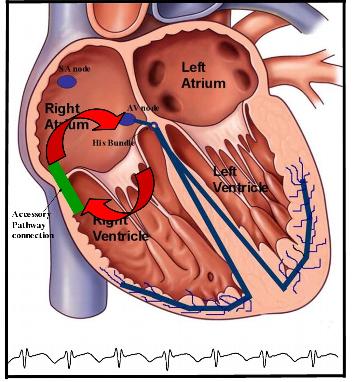 Figure 3. Illustration of orthodromic atrioventricular reciprocating tachycardia (AVRT) with a reentrant circuit consisting of 2 limbs. The forward or antegrade limb involves the normal AV nodal system, and the reverse, or retrograde, limb involves the accessory pathway. This type of SVT leads to a narrow-complex rhythm on the EKG as seen above.
Figure 3. Illustration of orthodromic atrioventricular reciprocating tachycardia (AVRT) with a reentrant circuit consisting of 2 limbs. The forward or antegrade limb involves the normal AV nodal system, and the reverse, or retrograde, limb involves the accessory pathway. This type of SVT leads to a narrow-complex rhythm on the EKG as seen above.
In a similar fashion, the electrical conduction can occur in the reverse direction as described above. In this situation, an antidromic AVRT can occur with electrical conduction of the sinus impulse via the preexcited accessory pathway (antegrade fashion), and then retrograde via the normal AV node to create a circuit reentry rhythm. This form of SVT leads to a wide-complex fast heart rhythm and is much less common than the narrow form of orthodromic AVRT.
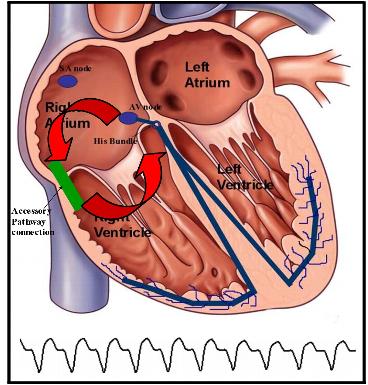 Figure 4. Illustration of antidromic atrioventricular reciprocating tachycardia (AVRT) with a reentrant circuit consisting of 2 limbs. The forward, or antegrade, limb involves the accessory pathway, and the reverse, or retrograde, limb involves the normal AV nodal conduction system. This type of SVT leads to a wide-complex rhythm on the EKG as seen above.
Figure 4. Illustration of antidromic atrioventricular reciprocating tachycardia (AVRT) with a reentrant circuit consisting of 2 limbs. The forward, or antegrade, limb involves the accessory pathway, and the reverse, or retrograde, limb involves the normal AV nodal conduction system. This type of SVT leads to a wide-complex rhythm on the EKG as seen above.
An antidromic tachycardia refers to a fast heart rhythm that utilizes the manifest accessorypathway to preexcite the ventricles, irregardless of whether the normal AV node is used in a retrograde fashion. In other words, other SVTs, such as atrial tachycardia or atrial flutter and fibrillation can now conduct at fast heart rates to the ventricles in a 1 to 1 fashion (no protection to limit this conduction since the AV node is not in use). This is the theoretical danger of an accessory pathway that allows conduction to the ventricles in an uncontrolled, potentially fast rate, with repetitive stimulation of the ventricles potentially leading to ventricular fibrillation with hemodynamic collapse and sudden cardiac death. This situation is rare and it is estimated that this tragic event has less than a 0.1% chance (1 in a 1000) of occurring each year in patients with manifest WPW.
Not all accessory pathways are manifest with a delta wave on the 12-lead EKG (no WPW EKG pattern seen). Concealed WPW is actually more common than manifest WPW. In these situations, the patient will have a normal baseline EKG but a clinical narrow-complex SVT of unclear origin. These accessory pathways are concealed may conduct only in the reverse, or retrograde fashion, leading to orthodromic AVRT as described above, but no clues to its existence with a normal baseline EKG. In addition, multiple accessory pathways are present in as many as 13% of patients referred to a heart rhythm specialist because of WPW syndrome.
Symptoms
The symptoms of AVRT are similar to other SVT, with palpitation, lightheadedness, dizziness, shortness of breath, reduced exercise capacity, weakness, fatigue, chest discomfort, and sweating episodes. These symptoms are primarily due to the development of rapid and/or irregular ventricular rates.
Diagnosis
Atrioventricular reciprocating (AVRT) tachycardia can be diagnosed by your physician via an electrocardiogram or an ambulatory monitoring device, i.e. Holter or Event monitor, specifically during an arrhythmia episode. These episodes of SVT can be intermittent and not reliably present on a daily basis. In these situations, your physician may recommend a special ambulatory monitoring device that is patient-triggered, i.e. an Event monitor. Because ambulatory monitoring devices, such as Holter monitors and Event monitors are only able to record one or two EKG leads, this may make discrimination of AVRT from other SVT difficult. In addition, the 12-lead EKG of AVRT can be difficult to differentiate from other SVT, particularly AVNRT. For patients who require an unequivocal diagnosis, or are candidates for a “curative” catheter ablation procedure, an intracardiac electrophysiology study is the “gold standard” test to establish the diagnosis (see below).
Prognosis
Some patients are able to reduce their symptomatic episodes with life-style modification, including avoidance of caffeinated beverages, alcohol, sleep-deprivation, stressful situations, and anxiety. The frequency or severity of symptoms may fluctuate from time-to-time, but they rarely disappear. Because the arrhythmia is due to an abnormal electrical circuit in the heart, there is little any patient can do by himself or herself to prevent or suppress the arrhythmia completely.
As discussed earlier, the diagnosis of SVT is virtually never life-threatening. The one exception to this rule involves the very rare patients with manifest WPW. It is these patients who may develop 1 to 1 conduction from the atria to the ventricles via the accessory pathway during an atrial tachyarrythmia such as atrial tachycardia or atrial fibrillation. With atrial fibrillation, the atria can contract at rates faster than 300 beats per minute. With the potential for conduction in nearly a 1 to 1 fashion with a manifest accessory pathway, repetitive ventricular stimulation at these fast rates during atrial fibrillation can lead to ventricular tachycardia and fibrillation with the risk of sudden cardiac death. This situation is rare and it is estimated that this tragic event has less than a 0.1% chance (1 in a 1000) of occurring each year in patients with manifest WPW.
Therapy
Therapy for patients suffering from AVRT depends on the frequency and severity of symptoms. Your physician may decide to implement therapy with oral medications if you are having frequent episodes that affect your daily living. As well, your physician may ask you perform certain “vagal” maneuvers once an episode of AVRT appears, to help terminate it. The Valsalva maneuver, in which the patient takes a deep breath in, holds it, and then bares down as if they were having a bowel movement, is sometimes effective in terminating AVRT. Carotid massage, in which the patient presses and rubs on the region of the neck where the carotid pulse is most prominently felt, also may be helpful. However, this procedure must be done with care or avoided in the elderly, and in those patients with evidence of occlusive carotid artery disease and bruits (please consult your physician).
 Medication is far and away the most common first-line treatment option. Medications used to terminate symptomatic AVRT episodes and to reduce occurrences include b-blockers, calcium channel blockers, and antiarrhythmic drugs. These medications can be administered orally on a routine outpatient basis, or via intravenous route if necessary in the emergency room. Some patients may need a combination of medications from different classes. The antiarrhythmic medications are not without risks, with potential side effects that require specific counseling with your physician. Drug response is variable and highly individualized, with some patients responding and others not. It is a trial and error proposition, with no possibility of knowing what would be most effective for each individual patient ahead of time. Treatment of symptomatic episodes of AVRT is difficult on an outpatient basis for those patients who do not wish to take a daily regimen of medications. Oral medications take at least a couple of hours to be absorbed, by which time most paroxysms of AVRT self-terminate, terminate with vagal maneuvers performed by the patient, or are symptomatic enough to prompt an ER visit with IV medications used to terminate the episode.
Medication is far and away the most common first-line treatment option. Medications used to terminate symptomatic AVRT episodes and to reduce occurrences include b-blockers, calcium channel blockers, and antiarrhythmic drugs. These medications can be administered orally on a routine outpatient basis, or via intravenous route if necessary in the emergency room. Some patients may need a combination of medications from different classes. The antiarrhythmic medications are not without risks, with potential side effects that require specific counseling with your physician. Drug response is variable and highly individualized, with some patients responding and others not. It is a trial and error proposition, with no possibility of knowing what would be most effective for each individual patient ahead of time. Treatment of symptomatic episodes of AVRT is difficult on an outpatient basis for those patients who do not wish to take a daily regimen of medications. Oral medications take at least a couple of hours to be absorbed, by which time most paroxysms of AVRT self-terminate, terminate with vagal maneuvers performed by the patient, or are symptomatic enough to prompt an ER visit with IV medications used to terminate the episode.
For those patients who elect to forgo medication either due to
- intolerable symptoms or side effects from their medications,
- recurrent symptoms and episodes despite medical therapy,
- lack of desire to take daily medications for an extended period of time, or
- “high-risk” accessory pathway conduction
your physician may recommend you undergo an electrophysiology study (EPS) and possible “curative“ catheter ablation. In brief, these procedures are performed in a special procedure room called an electrophysiology (EP) laboratory. The EP laboratory houses a table and an x-ray (fluoroscopy) machine that is suspended over the table. With the use of specialized electronic and computer equipment, in conjunction with the intracardiac electrode catheters (placed into the heart via the femoral veins), your heart rhythm specialist will use fluoroscopic and electrical guidance to map and deliver radiofrequency energy to the accessory pathway, thus eradicating the rhythm disturbance.
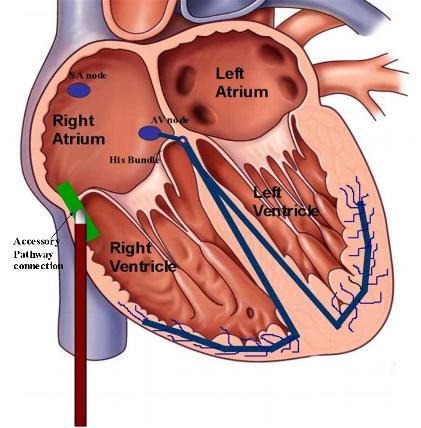 Figure 5. Illustration of catheter ablation of an accessory pathway. Using intracardiac mapping techniques, the location of the accessory pathway is determined. The tip of the ablation catheter is advanced to the area and the local tissue is heated with radiofrequency energy to eradicate the accessory pathway.
Figure 5. Illustration of catheter ablation of an accessory pathway. Using intracardiac mapping techniques, the location of the accessory pathway is determined. The tip of the ablation catheter is advanced to the area and the local tissue is heated with radiofrequency energy to eradicate the accessory pathway.
Radiofrequency energy employed during the catheter ablation procedure heats the tissue enough to destroy the local heart cell function, but without physically cutting through the tissue. The long-term success rate for catheter ablation of accessory pathways is well above 90%. However, recovery of tissue function months to years later is possible as the heart attempts to heal itself, with a delayed return of accessory pathway conduction possible. These cases can be approached with a repeat ablation procedure with similarly higher success rates. The risk of serious complication, including complete heart block requiring implantation of a permanent pacemaker, is 1% or less, in those cases with an accessory pathway near the normal AV nodal system. The risks of radiofrequency catheter ablation are very small and will be discussed in detail with each patient by their heart rhythm specialist at the time of the initial office visit.
In the end, the patients who choose the catheter ablation procedure over no treatment or medical options have decided that the improvement in their quality of life resulting from elimination of the tachycardia (and cure) far outweigh the very small risks associated with undergoing the procedure.
- Arrhythmias
- Sick Sinus Syndrome
- Atrioventricular (AV) Block
- Atrial Tachycardia
- AV nodal reentrant tachycardia (AVNRT)
- Wolff-Parkinson White Syndrome (WPW) and Atrioventricular reciprocating tachycardia (AVRT)
- Atrial Flutter
- Atrial Fibrillation
- Cardioversion
- Ventricular Tachyarrhythmias
- Long QT Syndrome
- Sudden Cardiac Death (SCD)
- Syncope



 Silver Spring Office
Silver Spring Office  DC Office (at Providence Hospital)
DC Office (at Providence Hospital)  Hagerstown Office
Hagerstown Office